chronic decompensated liver disease secondary to alcoholism
This is an online E log book to discuss our patients deidentified health data shared after taking his/her/guardians signed informed consent.
Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problems with collective current best evidence based inputs.
This E log book also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
Here is a case I have seen :
Unit 6 admission :
Case admitted in male ward on 6/2/2021.
Interns
K.Divya Rachana
K. Nikhil reddy
M. Swarna
B.Manivarma
Juveria
Dr. Vinay(pgy1)
Dr. Rashmitha(pgy2)
Dr. A. Vaishnavi (pgy2)
Dr. Sai Radha(pgy3)
Dr. Hareen (SR)
Dr.Praveen Naik( asst.proff)
A 37 year old male resident of achanpally, who's a chronic alcoholic since 5 years,consumes brandy 80 ml/day,last alcohol intake is 9 days back came with complaints of
Right scrotal swelling 9 days back,got treated by a local doctor but not relieved.After 2 days patient noticed pedal edema, pitting type upto knee.He also complained of pain in the epigastric region, burning type associated with abdominal distension and shortness of breath.Shortness of breath increased on sitting but not on walking.Orthopnea absent.Tremors of both hands since 9 days.H/O of tremors 5 years ago whenever he stopped taking alcohol.No H/O of hemetemesis,Malena,loose stools, jaundice.No h/o oliguria, cough, fever, palpitations.
Past history-He gave a h/o burning sensation in feet 3 years ago,no tingling and numbness,no sensory loss and weakness.He also gave a history of jaundice 1 year back for which he was on medication for 15 days.No h/o dm,htn,CVD, epilepsy,asthma
Personal history-he consumes mixed diet with normal appetite, adequate sleep, regular bladder and bowel movements.. He's a chronic alcoholic since 9 years.he consumes 80 ml of brandy every day..
On examination patient is conscious, coherent and cooperative
Pedal edema-grade II, pitting type.
Bp-130/80 mm of hg
PR-102 bpm
CVS-S1,S2 heard,no murmurs
RS-bae+
P/A-
On inspection
Abdomen distended, umbilicus everted and flanks full, horizontal scar 5 cm above umbilicus of size 7*2 cms
On palpation-splenomegaly +,no tenderness
On percussion-shifting dullness +,b/l flanks-dull note
On ascultation-bowel sounds heard
Provisional diagnosis-chronic decompensated liver disease secondary to alcoholism.
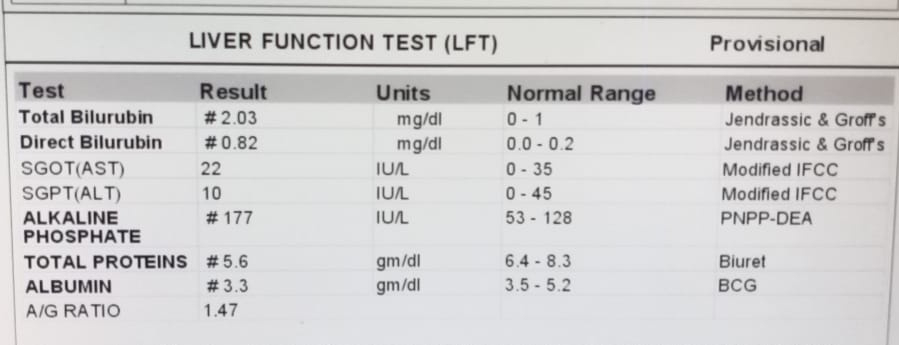
Investigations :


















Treatment day 1:
1.Fluid restriction <1.5 lit day
2.Salt restriction < 2g/ day
3.Tab. Lasilactone 20/50 mg PO/OD
4.Inj. Thiamine 1 amp in 100 ml NS/ Iv /BD
5.Bp charting 4 th hrly
Treatment day 2:
1.Fluid restriction <1.5 lit day
2.Salt restriction <2g/day
3.Tab. Lasilactone 20/50 mg PO/OD
4.Inj. Thiamine 1 amp in 100
ml NS/ Iv /BD
5.Bp charting 4 th hrly
6.Tab. Oxazepam 30 mg for 2 days
7Tab. PAN 40 mg PO/OD BBF at 8 am.
8.Protein powder 2 tsp in 1 glass of milk PoTID
9.T. PCm 650 mg PO/SIS
10.Syp. Sucralfate 10 ml PO/OD 20 mins BF
11.Syp. LACTULOSE 10 Ml PO/TId
12.Inj. Ceftriaxone 1 gIVBD after test dosing. 13.Tab. Rifaximin 550 mg PO/BD
14.BP,PR,RR ,SPo2 charting 4 th hrly
Treatment day 3:
1.Fluid restriction <1.5 lit day
2.Salt restriction <2g/day
3.Tab. Lasilactone 20/50 mg POOD
4.Inj. Thiamine 1 amp in 100
ml NS/ Iv /BD
5.Bp charting 4 th hrly
6. Tab. Oxazepam 30 mg for 2 days
7.Tab. PAN 40 mg POOD BBF at 8 am.
8.Protein powder 2 tsp in 1 glass of milk PoTID
9.T. PCm 650 mg POSIS
10.Syp. Sucralfate 10 ml POOD 20 mins BF
11.Syp. LACTULOSE 10 Ml POTId
12.Inj. Ceftriaxone 1 gIVBD after test dosing. 13.Tab. Rifaximin 550 mg POBD
14.BP,PR, RR ,SPo2 charting 4 th hrly